Researchers continue to hone in on the best way to use MRI for patients suspected of having prostate cancer, and AI is helping the effort. A new study in AJR shows that AI can improve the diagnostic accuracy and consistency of prostate MRI – while making it easier to perform.
Multiparametric MRI is the gold standard for prostate cancer imaging, but requires the use of three different MRI sequences as well as contrast administration, making it more complex and time-intensive to perform.
- On the other hand, biparametric MRI uses just two sequences – T2-weighted and diffusion-weighted imaging – and omits the contrast entirely, leading to shorter scan times and lower cost.
But what are you losing with bpMRI – and can AI help you get it back? Researchers addressed this question in the new study in which six radiologists interpreted bpMRI scans of 180 patients from multiple centers.
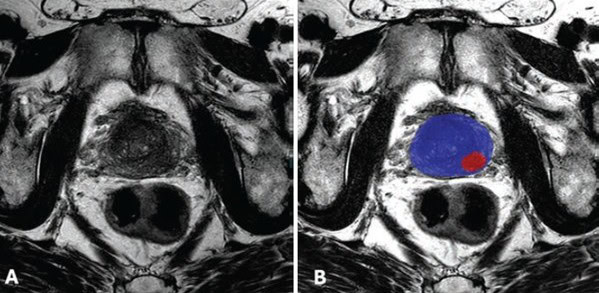
- Radiologists used a deep learning algorithm developed at the NIH to interpret bpMRI scans acquired on 3T scanners. The open-source algorithm generates binary prostate cancer prediction maps that are overlaid on T2-weighted images.
Researchers found that radiologists using the bpMRI AI algorithm to detect clinically significant prostate cancer had…
- An increase in lesion-level positive predictive value (77% vs. 67%).
- But lower lesion-level sensitivity (44% vs. 48%).
- And no statistically significant difference in patient-level AUC (0.82 vs. 0.83, p = 0.61).
- While inter-reader agreement scores improved for lesion-level and patient-level PI-RADS scores and lesion size measurements.
What to make of the numbers? The authors pointed out that the study design – in which AI was used as a first reader – may have reduced AI’s performance.
- In real clinical practice, AI would most likely be used as a sort of clinical spell checker, with AI results overlaid on images that radiologists had already seen.
The researchers said the results on improved positive predictive value and inter-reader agreement show that AI can improve the diagnostic accuracy and consistency of bpMRI for prostate cancer.
The Takeaway
The new findings echo other research like the PI-CAI study highlighting the growing role of AI in prostate cancer detection. If validated with other studies, they show AI-assisted bpMRI could be ready to take on mpMRI for a broader role.








